Download
1 / 33
340 likes | 371 Views
Hemoflagellates of medical importance. Leishmania spp. & Trypanosoma spp. have digenetic life cycles, involving vertebrate hosts (Man & reservoir animals) and invertebrate hosts (arthropods) . There are 4 parasitic stages (or forms):

E N D
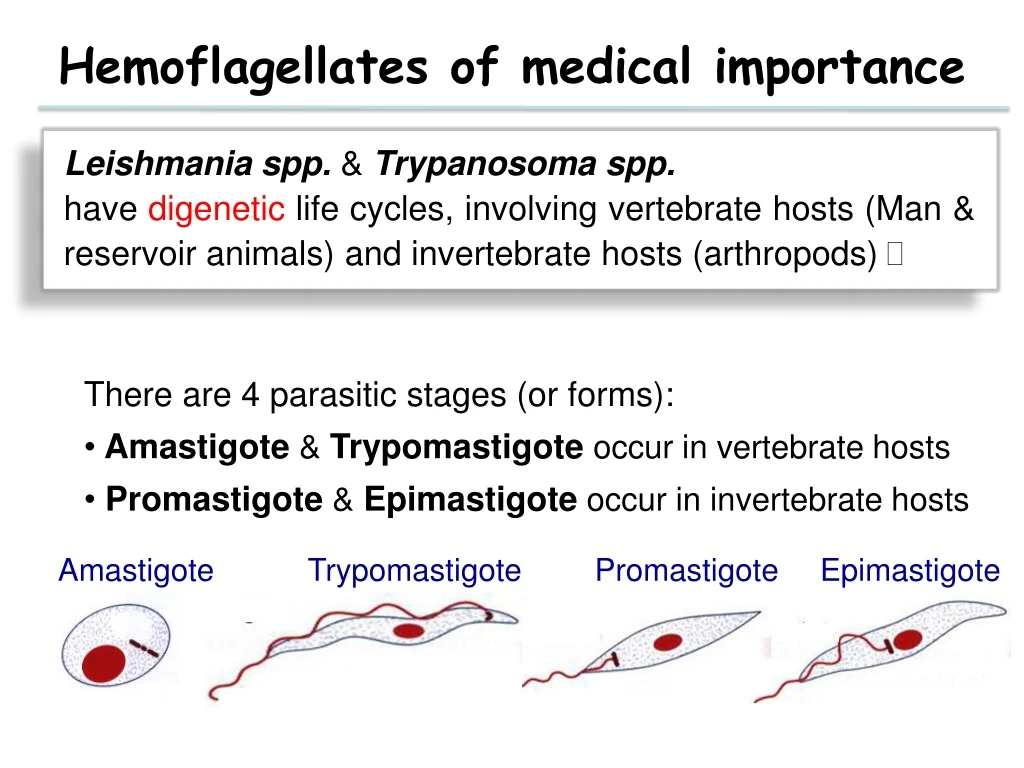
Hemoflagellates of medical importance Leishmania spp. & Trypanosoma spp. have digenetic life cycles, involving vertebrate hosts (Man & reservoir animals) and invertebrate hosts (arthropods) • There are 4 parasitic stages (or forms): • Amastigote & Trypomastigote occur in vertebrate hosts • Promastigote & Epimastigote occur in invertebrate hosts Amastigote Promastigote Epimastigote Trypomastigote
Genus:LeishmaniaDisease: Leishmaniasis. Leishmaniasis • Leishmaniasis is classified according to its clinical picture & geographical distribution: • I- Cutaneousleishmaniasis • A- Old World Cutaneousleishmaniasis. • B- New World Cutaneousleishmaniasis. • II- Mucocutaneousleishmaniasis • A- New World Mucocutaneousleishmaniasis. • III- Visceral Leishmaniasis. • A- Old World Visceral leishmaniasis. • B- New World Visceral leishmaniasis. • --
Geographical distribution of cutaneous leishmaniasis in Saudi Arabia.
Most common form(s) of Leishmaniasis. Cutaneous Leishmaniasis Infective stage Promastigote or Amastigote. Transmission 1-Biological: Bite of infected female ♀ sand flies. (Infective stage >>> Promastigote form). 2-Mechanical: Direct contact andautoinfection. (Infective stage >>> Amastigote form).
Vector Female sand flies Male Female
Life cycle of Leishmania [Cutaneous and Mucocutaneous]in humans and reservoir animals
Life cycle of Leishmania species The infective stage is transmitted by the bite of blood-feeding female sand flies (Phlebotomus or Lutzomyia) which carries the promastigote in the anterior gut and pharynx. It get engulfed by local macrophages where it transform into amastigotes and divides until the infected cell ruptures. The released organisms infect other cells. The sand fly acquires the organisms during its meal, the amastigotes transform into flagellate promastigotesand multiply in the gut until the anterior gut and pharynx are packed. Salivary glands are not invaded.
C/P of Cutaneousleishmaniasis Clinically differs according to the species of the parasite & the immunity of the patient • Old World CL: caused by L. tropica complex (L. tropica, L. major & L. aethiopica). • New World CL: caused by L. mexicana& L. braziliensis complexes. Classical lesion The lesion starts at the site of insect bite as a Papule >>> Nodule; due to multiplication of Leishmania formin skin macrophages followed by granulomatous reaction around them; then >>>ulcerates and the ulcer heals leaving a disfiguring scar.
A- Old World Cutaneous LeishmaniasisL. tropica complex Leishmania tropica causing Chronic, dry or urban CutaneousLeishmaniasis: Painless ulcer or Oriental sore. Leishmania major causing Acute, wet or rural Cutaneous Leishmaniasis. Leishmania aethiopica Causing Diffuse (Disseminated) CutaneousLeishmaniasis.
Chronic, Dry or Urban OWCL [caused by L. tropica]. Reservoir host: Dogs. Incubation period: 2-8 months. Distribution: Occurs in Mediterranean region, Middle East, parts of Africa & Asia (mainly in urban areas). It give the following lesions:
Painless ulcer orOriental sore • The lesion starts as a single red prurtic papule on the exposed parts of the body. • It is dry, painless, increases in size, ulcerates and crusts after several months. • The ulcer [Oriental sore] has sharp cut edges, raised indurated margin (volcano like), with scanty exudates. • 2nd bacterial infection may occurs. • Healing takes place spontaneously in about 1-2 years leaving depigmented flat, atrophic, disfiguring scar. • parasites are seen only in the edges • This lesion is common in Saudi Arabia.
Acute, Wet or Rural OWCL [caused by L. major] Reservoir host: Rodents. Incubation period: 2-6 weeks. Distribution:Occurs in the desert areas of Middle East, Asia, Africa [mainly in rural areas]. It is common in Saudi Arabia The Lesions are multiple, painless, severely inflamed, moist with serous exudates and rapidly ulcerating. 2nd bacterial infection is common. Healing takes place within 3-6 months, leaving large disfiguring scars.
Diffuse; Disseminated; Cutaneous Leishmaniasis [Caused by Leishmania aethiopica] Distribution: L. aethiopica occurs mainly in Ethiopia, Kenya & south Yemen. The parasite causes chronic form with late ulceration but is usually proliferate indefinitely [due to deficient cell-mediated immunity] Producing Diffuse Cutaneous Leishmaniasis
Diffuse; Disseminated; Cutaneous Leishmaniasis [Cont.]. It takes the form of widely disseminated thickening of the skin (papules or multiple non ulcerative nodules) on the face & exterior surface of limbs. The lesion is non self healing & similar to Lepromatous leprosy
B- New world cutaneous and mucocutaneousleishmaniasis [NWCL] Parasite: L. braziliensis complex & L. mexicana complex. Distribution: Occurs in Central & South America. Reservoir hosts: Forest rodents & dogs. Vector: ♀ Sand fly, genus Lutzomyia. The clinical features are similar to those of OWCL but lesions tend to be more severe & chronic.
B- New world cutaneous and mucocutaneous leishmaniasis [NWCL] [1] Leishmania braziliensis complex a. Mucocutaneous Leishmaniasis or Espundia: Caused by L. braziliensis. b. Uta: Caused by L. peruviana; Single or few painless skin ulcers that heal spontaneously. [2] Leishmania Mexicana complex a. Chiclero’s ulcer or Bay sore.
II- Mucocutaneous Leishmaniasis or Espundia Pathology & Clinical picture L. braziliensis produces single ormultiple lesions; Similar to oriental sore; that undergo extensive ulceration. After months or years, lymphatic spread to mucous membranes of nose, mouth & ear may occur >>> hypertrophy, destruction, severe pain & great deformity .
Mucocutaneous Leishmaniasis or Espundia [Cont.] Disfigurationis often extreme with complete destruction of the nasal septum, perforation of the palate and damage to the tissues of the lips and larynx. It is accompanied with fever, anaemia & loss of weight. Deathoccurs as a result of 2nd bacterial infections or malnutrition.
Chiclero’s ulcer or Bay sore Occurs in forest workers [Chicle collectors]. It is a single painless lesion mainly affects the ear causing destruction of cartilage & heal spontaneously within 6 months. Chiclero’s ulcer or Bay sore
Diagnosis of Cutaneous leishmaniasis • Clinical Diagnosis: - History: Residence or traveling to endemic area. - Clinical picture. II. Laboratory Diagnosis 1- Direct Methods. 2- Indirect methods: a- Intradermal skin test [Leishmanin or Montenegro's test]: It is a delayed hypersensitivity skin test. Positive test [˃ 95%] >>> induration more than 5 mm at site of injection after 48 hours. It is –ve in D.C.L. (since there is deficiency in cell mediated immunity). b- Aspirate or biopsy >>> PCR to diagnose & type the species. Killed Leishmania from culture (leishmanin antigen) are injected in the arm
1- Direct Laboratory Methods Amastigote a-Aspirated tissue juice, scraping or biopsy material from raised nodule or raised edge of the ulcer & from mucosal scraping in mucocutaneous type to detect the parasite after: preparing smears & staining with Giemsa or Leishman stains >>>Amastigote form. b- Inoculation in culture [NNN medium] >>> Promastigote form. c-Animal inoculation >>Amastigote form. Promastigote
Aspiration and biopsy from the ulcer Scrape or take biopsy Aspiration Leishmania amastigotes (Giemsa stained)
Laboratory Diagnosis Sample collection From the edge of the ulcer
Treatment 1- Non inflamed-non ulcerated lesion: Intra- lesional injection of pentavalent antimonial or 5% mepacrine, 1-3 times at 3-5 days interval. 2- Inflamed or ulcerated lesions, multiples lesions, or lesions on sites where scarring might produce disability or disfigurement: Pentostam I.V or I.M., 10:20 mg/kg/day for 10 days. 3- I.D. injection of interferon gamma around the lesion to promote healing of the ulcer. 4- Antibiotics: for 2nd bacterial infections 5- Local application of heat to 37- 43 ºC. 6- Surgical removal, CO2 snow or X-ray.
Prevention & control 1-Treatment of cases, control of vector & reservoir hosts. 2- Proper dressing of the ulcer [Why ???]. 3-Active immunization on concealed parts of body in endemic areas. 4- Protection: by using wire screens, repellents & mosquito nets
Leishmaniasis in KSA L. major L. tropica L. infantum
